

Clinical trials depend on evidence. Not only evidence that a treatment works, but evidence that the instruments used to measure its effects are asking the right questions, in the right way, and producing scores that can be interpreted with confidence.
Developing a clinical outcome assessment (COA) is therefore very different from writing a survey questionnaire. It is a structured process of defining what should be measured, gathering evidence that the content represents the intended construct, demonstrating that scores are reliable and meaningful, and showing that the instrument is appropriate for the population and purpose for which it will be used.
This process did not originate in the clinical research community. It is grounded in psychometrics and decades of psychological, educational and health measurement science. And it is reflected in internationally accepted test development standards that are not governed by the same regulators that govern pharmaceutical manufacturing and clinical development.
The world’s major regulators, including FDA, EMA, Health Canada, PMDA, NMPA, and CDSCO, draw on these principles into their guidance documents and review processes, although they differ in how explicitly they describe the evidence they expect and the flexibility they allow.
For test developers, this has important implications. Instruments developed primarily for clinical practice, education, or research may not provide the evidence or flexibility needed for today’s multinational clinical trials. As sponsors increasingly seek assessments that can support regulatory decision-making across countries and populations, test developers have an opportunity to rethink not only how instruments are developed, but how they are documented, maintained, and adapted throughout their lifecycle.
Nothing about us, without us.
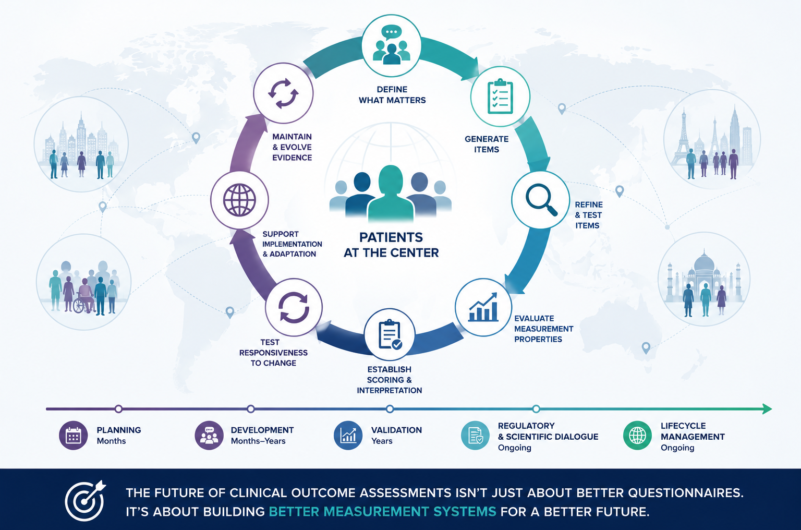
A clinical outcome assessment begins with the people whose health or functioning it is intended to represent, together with the patients, clinicians, caregivers or observers who can provide the relevant information.
Developers need to understand what matters to them, how they describe it, and which changes would be meaningful in daily life. That evidence helps define the construct, the target population, the appropriate respondent or rater, and the interpretation the scores are expected to support.
In clinical trials, those scores may be used to show whether a treatment improves symptoms, functioning, cognition, or quality of life. The intended use shapes the content of the instrument.
This principle is well established in test development standards and reflected across regulatory guidance. The language varies, but the expectation is consistent: the instrument must be grounded in the population for whom it is being developed.
If the target population is not clearly defined, then content validity is not be clearly established.
From conversations to questions
Listening to patients is only the beginning.
The challenge is translating their experiences into questions that are relevant, understandable, and capable of producing meaningful scores.
Developers typically begin with a broad pool of candidate items drawn from patient interviews, clinical expertise, existing instruments, and scientific literature. Those items are refined through multiple rounds of review, cognitive interviews, and pilot testing to determine whether respondents interpret them as intended.
The development history and supporting data are as valuable as the final questionnaire. Years later, they may be needed to justify revisions, translations, electronic implementation, or use in another population.
The development history and the data sets are just as valuable as the final questionnaire. Understanding why an item was revised, retained, or removed can become important years later when an instrument is adapted for a new indication, target population, implemented electronically, translated into another language, or evaluated for use in multinational clinical trials.
Building confidence in the scores
By this stage, the instrument has a defined purpose, a conceptual framework, and a refined set of items. The next step is to determine whether the scores can support the interpretations the developer intends to make.
This is where measurement science comes in.
The evidence may include reliability, structural validity, relationships with other measures, responsiveness to change, measurement invariance, or modern psychometric approaches such as Item Response Theory (IRT). The choice of methods depends on the instrument and the questions being asked.
No single statistical analysis can establish that an instrument is “valid.” Instead, each study contributes another piece of evidence showing that the scores behave as expected in the intended population and context of use.
The world’s major regulatory agencies follow the same principle. They generally do not prescribe a single psychometric approach or a single set of statistical thresholds. The methods and decision criteria must be justified for the proposed interpretation and context of use.
The scientific record should include item-level analyses, scoring decisions, revision evidence, and the rationale for the final model.
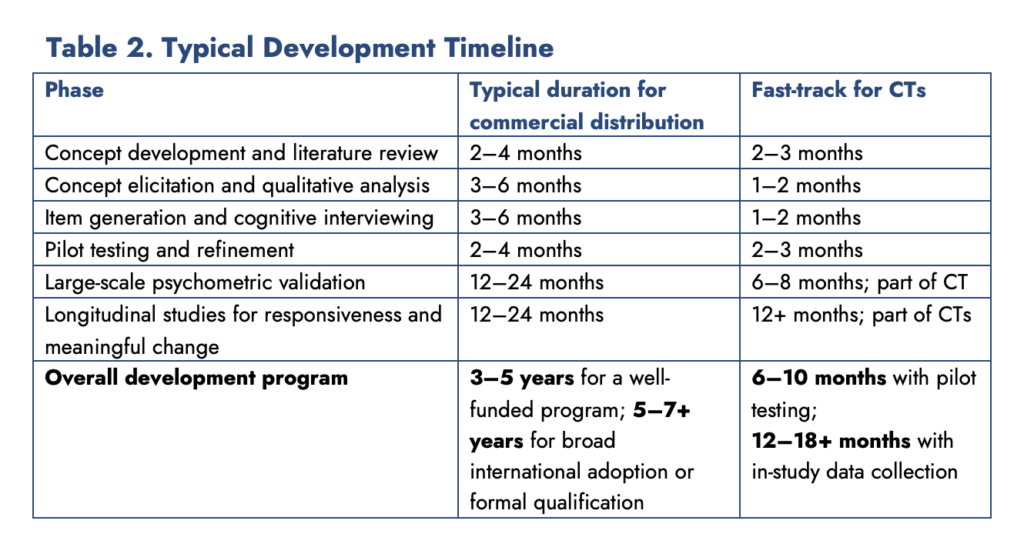
What does a typical COA development program look like?
These figures are planning ranges drawn from common psychometric practice, rather than regulatory minimums. Appropriate sample sizes depend on the instrument, target population, study objectives, statistical model, subgroup analyses and required precision.
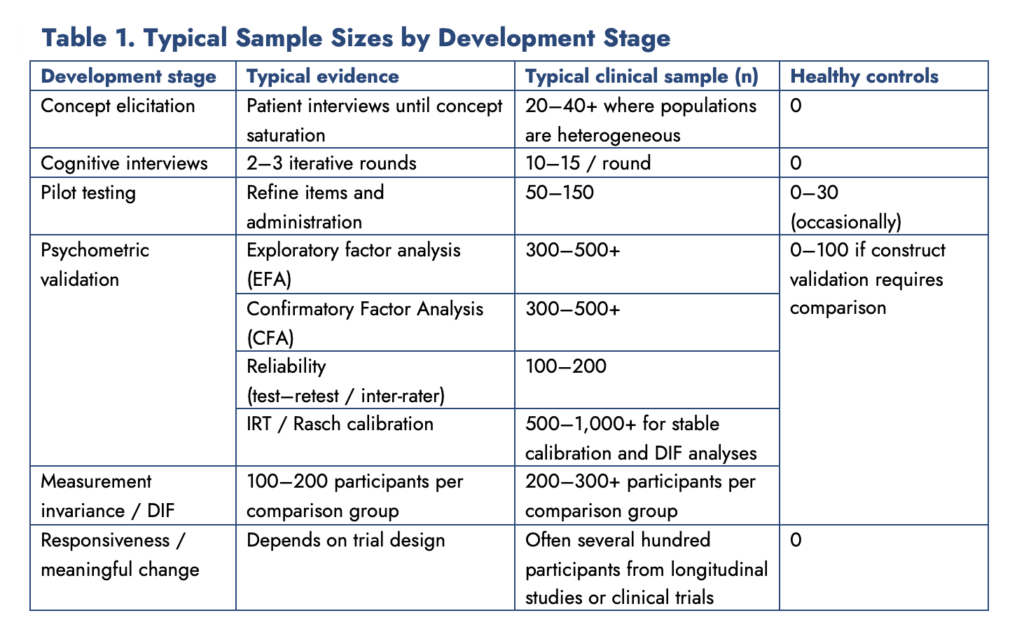
These sample sizes are not additive. A well-designed validation program can answer multiple measurement questions from the same study population.
Sample-size requirements vary with the construct, population, model, and intended analyses, but the ranges above provide a practical starting point for planning. They are not universal regulatory minimums, and the same study may support several analyses.
Can it detect change?
Clinical trials are built around treatment schedules. Research teams often want assessment timing to follow dosing, but recall period, administration frequency, and test–retest interval are not interchangeable.
Many instruments were validated using fixed intervals. Changing them may affect responsiveness or alter the interpretation of longitudinal scores.
Developers can anticipate this by evaluating more than one evidence-supported schedule during development.
Sensitivity to change in the real world
Clinical trials are built around treatment schedules.
A treatment may be administered every week, every two weeks, monthly, or at completely irregular intervals. Clinical research teams naturally want assessments to follow those schedules.
That usually creates a challenge with commercially designed measures.
Many instruments were developed using fixed recall periods and specific test-retest intervals. Those intervals support the original evidence for reliability and responsiveness. Changing them may seem like a small adjustment, but it can easily alter the instrument’s sensitivity to change. Sometimes, completely eliminate it.
The same issue arises when sponsors ask to shorten an assessment, administer only selected domains, migrate it to an electronic platform, or modify the instructions to fit a study protocol.
Some changes have little impact, but others require new qualitative work, additional psychometric evidence, or bridging studies before the scores can be reliably interpreted.
For developers, this represents an opportunity.
Instruments could be designed with documented adaptation pathways and validated modular or domain-level scoring options. Recall periods, administration schedules, electronic implementations, and approved modular forms could be evaluated during development, allowing future trial teams to work within evidence-based boundaries rather than starting from scratch.
COAs must evolve without losing their identity
Few clinical outcome assessments remain unchanged after publication. New evidence accumulates, technology changes, translations are added, populations shift, and new editions are released.
These changes are expected. The Standards for Educational and Psychological Testing call for periodic review of an instrument and the evidence supporting its interpretations and uses. Major restandardization is often considered over a period of approximately 20 to 25 years as cultural, ethnic, linguistic and demographic changes make an earlier standardization sample less representative.
Translations require the same attention. Language changes, terminology dates, and the populations using a translated version may also change. A translation approved 20 years ago is unlikely to remain appropriate simply because the source instrument has not changed.
In multinational studies, teams need to know what changed, why it changed, and whether scores remain comparable. Version histories, development records, translations, electronic implementations, and supporting evidence should remain accessible throughout the instrument’s lifecycle.
Global trials require global evidence
Multinational trials expect the same instrument to measure the same construct across countries, languages, healthcare systems, and cultural settings.
That is a demanding assumption.
Translation preserves language. Validation preserves measurement. Instructions, examples, response options, recall periods, and culturally specific concepts can all affect how an item functions. Accurate wording alone does not establish comparable measurement.
Evidence may include linguistic validation, respondent testing, qualitative research, measurement-invariance analyses, differential item functioning, or additional studies in the target population.
International use is rarely considered during original design. A source instrument developed with future adaptation in mind gives sponsors a stronger foundation for multinational research and gives publishers access to a broader market.
Designing for flexibility without compromising standardization
Clinical trial protocols may require electronic administration, selected domains, shorter forms, revised instructions, or alternative assessment schedules.
Each change raises the same question:
Can the instrument be adapted without changing what it measures?
Historically, many standardized assessments were designed as fixed products. Any modification was discouraged because it risked changing score interpretation.
That approach protected standardization, but it also limited flexibility.
Developers can build controlled flexibility into new instruments by creating modular structures, integratable electronic implementations, alternate test-retest schedules, and defined adaptation pathways while the evidence base is still being established.
Flexibility does not mean unlimited customization. Each supported variation needs evidence that scores remain interpretable and comparable.
Don't wait until the new instrument is finished
Evidence accumulates over time, which makes early scientific and regulatory dialogue useful when an instrument is intended for pivotal trials or regulatory submissions.
Available routes differ by jurisdiction and may include formal qualification, scientific advice, consultation meetings, or discussion within a product-development programme.
The immediate objective is to determine whether the evidence plan can support the intended endpoint and score interpretation. Formal qualification is one route, not a prerequisite for every use.
Publishers can contribute as long-term evidence partners by supporting additional populations, technologies, translations, and implementations as the scientific record grows.
Better design creates better long-term value
Developing a new clinical outcome assessment requires years of work and substantial investment. Planning for future adaptations, international deployment, AI-driven analytics, implementation across advanced technologies, and new target populations increases the value of that investment.
Publishers gain access to a broader international market. Sponsors gain more adaptable, evidence-supported endpoints. And patients benefit from assessments designed for the realities of modern global research.
The scientific record should continue to grow long after the first edition is published.
Clinical trials need flexibility. Granted, measurement science requires control, but the future belongs to instruments designed to accommodate both.
How Santium Contributes to This Space
Santium supports instrument developers with international data collection, content validation, cognitive interviewing and multilingual evidence generation.
Modern COA development, selection and eCOA implementations increasingly depend on understanding how physicians, patients and caregivers address and describe symptoms, treatment experience, functioning, burden of illness, burden of care, and quality of life within their own linguistic and cultural frameworks.
Santium contributions to the Life Sciences industry are designed to support the global implementation of patient-centered endpoints and patient-facing research materials. We do this through multilingual patient and stakeholder interviewing, cross-cultural evidence gathering, local subject-matter expert engagement, and measurement-aware linguistic and cultural adaptation.
Drawing on expertise in psychometrics, thousands of linguistic validation projects, multilingual interviewing, and multinational study operations, Santium helps sponsors and researchers evaluate whether patient-facing concepts remain relevant, clinically meaningful, culturally appropriate, and operationally usable across languages, countries, and modes of administration.
Are you interested or work in the COA-related area of clinical research?
If you found this article interesting, follow me on LinkedIn or subscribe to this Adapting COAs the Right Way series, where we explore the psychometrics hiding under the hood and the translation methods for clinical outcome assessments – from simple rating scales to complex neuropsychological batteries. We introduce their constructs, design rules you need to know about, the importance of phrasing, concepts being measured, and how cultural nuance and age-based norms impact the translation and cultural adaptation process.
Join me in elevating the quality of COA translation through a psychometrically-driven perspective.
Stay connected and don’t miss the next edition!
About the Author
Monika Vance | Managing Director | SANTIUM
My work sits at the intersection of linguistics, scientific and medical translation, psychometric measurement, and multilingual operations, where terminology, usability, end-user experience, and regulatory context must align. I write about scientific and medical translations, psychometrics, languages, patient-centred research and the operational challenges that inevitably come with them. I also teach translators how to properly translate and validate complex psychometric instruments to hone their expertise in linguistic validation.

|
Thank you for signing up. |

References
American Educational Research Association, American Psychological Association, & National Council on Measurement in Education. (2014). Standards for Educational and Psychological Testing. AERA.
COSMIN Initiative. (2024). COSMIN methodology for evaluating the content validity of patient-reported outcome measures. https://www.cosmin.nl
DeVellis, R. F., & Thorpe, C. T. (2021). Scale Development: Theory and Applications (5th ed.). Sage.
European Medicines Agency. (2008). Reflection paper on the regulatory guidance for the use of health-related quality of life (HRQL) measures in the evaluation of medicinal products. EMA.
European Medicines Agency. (2020). Qualification of novel methodologies for drug development: Guidance to applicants. EMA.
Food and Drug Administration. (2009). Guidance for industry: Patient-reported outcome measures: Use in medical product development to support labeling claims. U.S. Department of Health and Human Services.
Food and Drug Administration. (2022). Patient-Focused Drug Development Guidance 1: Collecting comprehensive and representative input. U.S. Department of Health and Human Services.
Food and Drug Administration. (2022). Patient-Focused Drug Development Guidance 2: Methods to identify what is important to patients. U.S. Department of Health and Human Services.
Food and Drug Administration. (2023). Patient-Focused Drug Development Guidance 3: Selecting, developing, or modifying fit-for-purpose clinical outcome assessments. U.S. Department of Health and Human Services.
Food and Drug Administration. (2024). Patient-Focused Drug Development Guidance 4: Incorporating clinical outcome assessments into endpoints for regulatory decision-making. U.S. Department of Health and Human Services.
Food and Drug Administration. (2020). Clinical Outcome Assessment (COA) Qualification Program. U.S. Department of Health and Human Services.
Health Canada. (2023). Guidance document: Considerations for clinical trials. Health Canada.
International Council for Harmonisation. (2023). ICH E6(R3): Guideline for Good Clinical Practice. ICH.
International Test Commission. (2017). The ITC Guidelines for Translating and Adapting Tests (Second Edition). International Journal of Testing, 18(2), 101–134.
International Society for Pharmacoeconomics and Outcomes Research. (2024). ISPOR Good Practices for Outcomes Research. ISPOR.
National Medical Products Administration. (China). (2023). Technical Guidelines for Patient-Reported Outcomes in Clinical Trials. NMPA.
Pharmaceuticals and Medical Devices Agency. (Japan). (2023). Points to Consider for Patient-Reported Outcome Measures in Clinical Evaluation. PMDA.
Streiner, D. L., Norman, G. R., & Cairney, J. (2015). Health Measurement Scales: A Practical Guide to Their Development and Use (5th ed.). Oxford University Press.
Terwee, C. B., Prinsen, C. A. C., Chiarotto, A., et al. (2018). COSMIN methodology for evaluating the content validity of patient-reported outcome measures: A Delphi study. Quality of Life Research, 27, 1159–1170.

Monika Vance
Managing Director | SANTIUM
My work sits at the intersection of linguistics, scientific and medical translation, psychometric measurement, and multilingual operations, where terminology, usability, and regulatory context must align. I write about scientific and medical translations, psychometrics, languages, patient-centred research and the operational challenges that inevitably come with them. I also teach translators how to properly translate and validate complex psychometric instruments to hone their expertise in linguistic validation.





