

Translation & Reconciliation
Concept-focused forward and back translations of COA instruments, followed by expert-led reconciliation to resolve linguistic discrepancies, align conceptual meaning, and prepare each item for cognitive testing. This step supports measurement integrity before pilot testing.
Clinician Review & Harmonization
Subject-matter specialists review medically sensitive content, rating instructions, anchors, and test items to assess clinical appropriateness. Cross-language harmonization aligns terminology and item intent across dialects, supporting consistent examinee comprehension and score interpretation.
Cognitive Debriefing
Semi-structured interviews with native speakers from the target population to evaluate comprehension, cultural relevance, item content usability and performance. Feedback is analyzed to identify misunderstood concepts, ambiguous wording, and potential barriers to accurate self-reporting and observation.
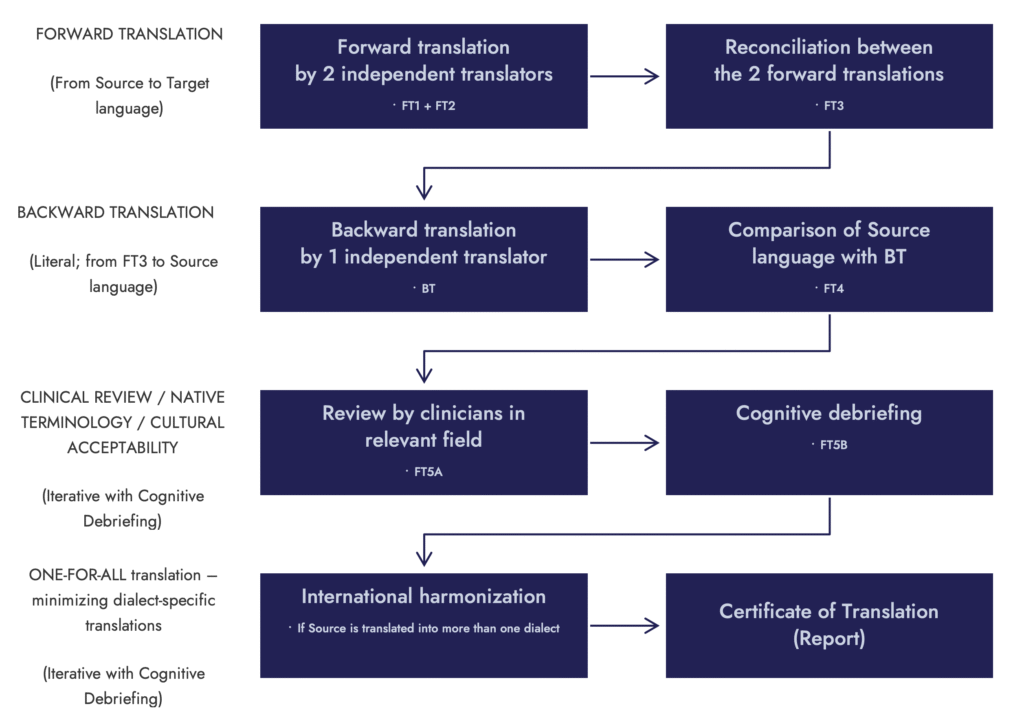
Cognitive Debriefing
Cognitive debriefing interviews test how real patients, caregivers, or clinicians understand translated COA items. Uncover problematic wording, cultural mismatches, and interpretation issues that affect usability. It is the second half of the Linguistic Validation method; without it, a translation is not linguistically validated.
Clinical Review & Editing
Native clinical specialists review medically sensitive concepts, rating instructions, anchors, and scoring guidance to assess clinical relevance and clarity. Editing focuses on refining terminology, resolving ambiguities, and aligning content with the intended clinical interpretation of each COA item and measurement concept.
Linguistic Review & Editing
Linguistic reviewers refine translated content by correcting terminology, resolving unclear phrasing, and improving structure while preserving the original meaning. Editing focuses on clarity, flow, and accuracy so materials read naturally and meet professional communication standards across scientific, medical, and technical domains.
Proofreading
We perform final quality checks to correct surface-level issues such as grammar, spelling, punctuation, formatting, and typographical errors. Proofreading ensures polished, error-free materials that are ready for publication, distribution, or regulatory submission, complementing earlier editing stages and maintaining consistency across related deliverables.
Glossary & Terminology
We build and maintain specialized terminology databases to unify language across subject-matter, studies and product lines. Controlled vocabularies reduce ambiguity, speed up editing time and strengthen quality assurance throughout the translation lifecycle.

Desktop Publishing
We maintain formatting integrity and brand recognition with polished professional layouts created by native-speaking designers and proofread by an independent reviewer. Translations are clear, accurate, with consistent formatting across manuals, forms, charts, and multi-page technical or scientific documents.

Dedicated Translation Teams
Small project-specific multi-disciplinary groups.

Translation Experience
Training and experience in COA translation.
Translatability Assessment
Pre-translation review that identifies linguistic and cultural conflicts before localization begins. This process reduces revision cycles by clarifying and defining ambiguous concepts, resolving inconsistencies in terminology, and identifying content that is not translatable and requires alternate wording, deeper adaptation or transcreation.
Clinimetric Review
Specialized expert review of outcome measures to support adaptation across languages, cultural contexts, and administration modes. To minimize noise in study data, we assess conceptual fidelity, scoring implications, and cross-cultural alignment to keep translated measurement items psychometrically sound and contextually relevant.
Translation & Localization
Clear, accurate, and domain-specific translation for clinical, scientific, technical, and corporate materials. All translations are produced by qualified subject-matter experts and reviewed for terminology accuracy, style consistency, and audience appropriateness, ensuring clarity and usability across languages and regions.
Data Collection & Validation
Cross-language validation of clinical outcome measures for new target populations, usability systems, and instructional content that supports relevant functional use, and target-audience comprehension. It also supports regulatory expectations and a consistent user experience across countries, languages and cultural contexts.
e-Learning Translation
High-quality translations for training content, rater modules, onboarding courses, and examination materials. Lessons, assessments, and interactive elements are localized for clarity, usability, and cultural relevance, helping global study teams deliver consistent learning experiences across sites, languages, and user groups.

Video Subtitling & Closed Captions
Precise, well-timed subtitles and closed captioning support multilingual training content, including onboarding videos, e-learning modules, and SOP walk-throughs. Terminology and procedural language are translated clearly so multilingual teams can follow demonstrations with ease.
Voiceover Translation (Dubbing)
Transcription, subtitling, voiceover, script localization, video production, and UX review for multimedia used in multi-language training, recruitment and onboarding, education, and research.
Transcription
Accurate, polished and secure transcription for clinical, scientific, and technical content. Audio and video files are converted into clean, structured text that is ready for analysis, review, and multilingual adaptation. Ideal for e-Learning content, training materials, interviews, high-impact meetings, presentations and documentation needing archiving or long-term knowledge retention.

Software Localization
Software localization for eCOA platforms supports your digital assessments, screens, and patient workflows feel native in every language. We adapt UI labels, messages, notifications, and task logic so they stay consistent and aligned with your requirements. Our team understands character limits, branching, scoring dependencies, and audit needs in eCOA systems, delivering a seamless experience across devices.
Video Production
Video production for COA training materials, patient instructions, and site-readiness programs. We create clear, culturally relevant videos that simplify complex concepts, maintain protocol compliance, and support consistent administration across sites and languages. Ideal for onboarding raters, guiding patients and caregivers, and enhancing the usability of COA and eCOA workflows.

PRO: Patient-Reported Outcome
Patient-Reported Outcome Measures capture patients’ direct reports of symptoms, functioning, and treatment experience without clinician or caregiver interpretation. In linguistic validation, we evaluate conceptual clarity, comprehension, response scales, recall periods, and item functionality. This helps support meaningful interpretation of data sets collected across international research sites.
ClinRO: Clinician-Reported Outcome
Clinician-Reported Outcome Measures are completed by trained healthcare professionals based on clinical judgment, direct observation, or structured rating procedures. Linguistic validation focuses on the clarity and precision of rating instructions, anchors, diagnostic terms, and scoring rules so clinicians interpret and apply each item consistently across countries. We also assess terminology, task descriptions, and administration guidance for the target population and local clinical context.
ObsRO: Observer-Reported Outcome
Observer-Reported Outcome Measures capture information from caregivers or observers about behaviors and symptoms that patients cannot reliably self-report. Linguistic validation focuses on the clarity of observable concepts, reporting instructions, and caregiver decision-making, ensuring that items are interpreted as intended across languages and cultural contexts. We also evaluate administration burden, examples, and task demands to prevent misclassification or inconsistent observation in multilingual studies.

PerfO: Performance Outcome
Performance Outcome Measures assess a patient’s ability to complete standardized tasks that measure specific aspects of functioning, such as motor skills, cognitive processes, or physical capability. In linguistic validation, we review the clarity of task instructions, stimuli descriptions, timing requirements, and scoring methods to avoid unintentionally altering task difficulty or administration. We also identify phrasing and cultural factors that unfairly impact participants' understanding and performance.